Fuentes: “So just like Hitler imprisoned Gypsies, Jews, communists, you know, all of his political rivals, we have to do the same thing with women. … So they go to the gulag first. They go to the breeding gulags.”

|
[he/they] Queer, trans, disabled, disgruntled. Former librarian, future dust.
|
Fuentes: “So just like Hitler imprisoned Gypsies, Jews, communists, you know, all of his political rivals, we have to do the same thing with women. … So they go to the gulag first. They go to the breeding gulags.”




A lawsuit targeting a landmark disability law has received new life after nine states filed an update that seeks to undercut federal mandates that people with disabilities receive care in their communities.
Texas, Florida, and seven other states allege that the Biden administration’s 2024 update to Section 504 of the Rehabilitation Act of 1973 is unconstitutional — specifically, the requirement that states must fund services in the “most integrated setting.”

In December, the federal government escalated its efforts to dismantle established standards of care for transgender youth by proposing to deny Medicaid funding to children’s hospitals that provide gender-affirming care. The proposal is currently under review, with the public comment period ending Feb. 17.
If enacted, children’s hospitals will face an extraordinary and coercive choice: forgo essential funding streams and jeopardize pediatric care for all, or deny care to a small, vulnerable population that has no alternative. Nearly all children’s hospitals rely on Medicaid funding. For many, Medicaid patients make up 50% of their patient volume. This means that the HHS proposal would essentially act as a ban on gender affirming care.

A Beerwolf (Bärwolf, Werwolf) is a German folk-tale monster commonly known as a werewolf.
In a debate arranged by Philip of Hesse and the Elector of Saxony in 1539, when it appeared the Holy Roman Emperor Charles V was readying to attack the Lutherans, Martin Luther introduced the concept of Beerwolf to describe the Pope and the Emperor.
From the Wikipedia article “Beerwolf,” edited to remove footnotes and links to improve readability
In the context of resistance theory, the Beerwolf, “in contrast to a mere tyrant, not only broke the law, but overturned the entire moral order upon which it is based. All the subjects of such a ruler … had the right to resist and even to kill him and all his supporters”.
This post was originally published on November 11th, 2025. I've been spending some time reworking and cleaning up the Inkhaven posts I'm most proud of, and completed the process for this one today.
Today, Canada officially lost its measles elimination status. Measles was previously declared eliminated in Canada in 1998, but countries lose that status after 12 months of continuous transmission.
Here are some articles about the the fact that we have lost our measles elimination status: CBC, BBC, New York Times, Toronto Life. You can see some chatter on Reddit about it if you're interested here.
None of the above texts seemed to me to be focused on the actual thing that caused Canada to lose its measles elimination status, which is the rampant spread of measles among old-order religious communities, particularly the Mennonites. (Mennonites are basically, like, Amish-lite. Amish people can marry into Mennonite communities if they want a more laid-back lifestyle, but the reverse is not allowed. Similarly, old-order Mennonites can marry into less traditionally-minded Mennonite communities, but the reverse is not allowed.)
The Reddit comments that made this point are generally not highly upvoted[1], and this was certainly not a central point in any of the articles. It is a periphery point in all of the articles above at best. Toronto Life is particularly egregious, framing it like so:
"mis- and disinformation were factors in the outcome, which are partly due to pockets around the country with low vaccination rates."
This is, ironically, misinformation: true information framed in such a way to precisely give you the incorrect view of things.
In this post I will make two arguments: first, yes, it is the Mennonites that began (and are the biggest victims of) the biggest measles outbreak of the current century, and second, thinking of them as resistant to vaccination is actively harmful to the work of eliminating measles from Canada once again.
I've been following the measles outbreak closely for basically its entire duration, because I have a subscription to my local newspaper, the Waterloo Record. The writers there do frequent updates on the outbreak, often with higher quality and more detail than you get in the national papers. This is because Waterloo Region has a significant Mennonite population, so shit sometimes got real scuffed.
Like, over last spring, there were fairly regular advisories about local stores we shouldn't go into or quarantine if we did because someone with measles went in. One of them was the pharmacy across the street from the university campus, so that was fun.
Here is what the outbreak looks like, Canada-wide:
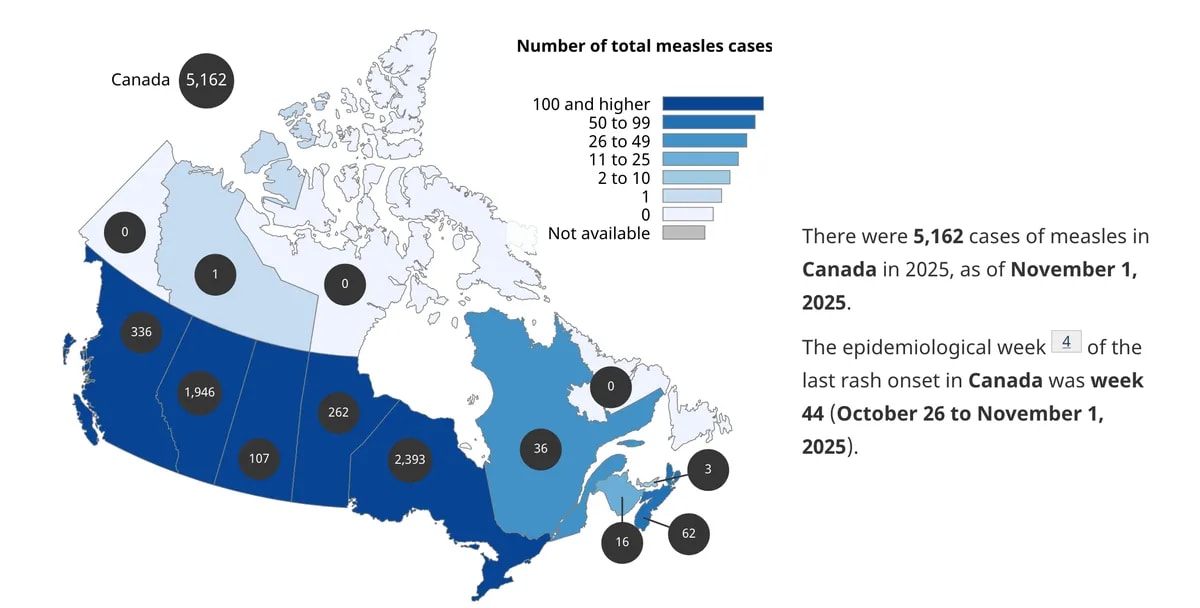
Full offense to Health Canada: this is a terrible graphic, because if you don't look at it carefully you will think that the provinces in dark blue have approximately the same number of cases, and this is very false. Sasksatchewan has barely over a hundred, Alberta has almost 2000, and Ontario has almost 2400 cases.
What's the deal with Ontario, and Alberta? Some of it comes down to the numbers game; those are two of our most populous provinces. But Quebec has twice the population of Alberta, and it's trucking on with only 36 cases in the entire province.
The answer is that it's the Mennonites, who are overwhelmingly settled in those two provinces.[2]
I'll be focusing on the outbreak in Ontario, because that's the part of the story I'm more familiar with. If you dig into older news pieces, the Mennonite connection is corroborated by government officials:
Previously, Moore [the Chief Medical Officer for Ontario] shared that this outbreak in Ontario was traced back to a Mennonite wedding in New Brunswick, and is spreading primarily in Mennonite and Amish communities where vaccination rates lag. The vast majority of those cases are in southwestern Ontario.
Mennonites have a social structure where, once the community reaches a certain number of families, they undergo mitosis, and half the families split off to form a new community far away. Based on reddit scuttlebutt, it seems like there has recently been a daughter community that moved from southern Ontario to New Brunswick, which makes it doubly unsurprising that there were many southern Ontario attendees to the original superspreader event.
Additionally, Moore, remarked in a memo he sent out to local health bodies:
Over 90% of cases in Ontario linked to this outbreak are among unimmunized individuals. Cases could spread in any unvaccinated community or population but are disproportionately affecting some Mennonite, Amish, and other Anabaptist communities due to a combination of under-immunization and exposure to measles in certain areas.
And Global News reports:
In an April interview with The Canadian Press [Moore] reasserted that the “vast majority” of Ontario’s cases are among people in [Mennonite, Amish, and other Anabaptist] communities.
Some smaller publications have found connections in their own investigation. The London [Ontario] Free Press in March 2025 (the beginning of the outbreak) linked the outbreak in West Texas to their Mennonite population, and identified that several measles exposure sites in counties that have been heavily afflicted by measles are Mennonite in nature:
A list of measles exposure sites in Grand Erie includes a church and several private Christian schools in western Norfolk County catering to Old Colony Mennonites, and Moore’s letter confirmed the link.
A recent Washington Post article also corroborates the link, but buries it under several paragraphs of preamble about general vaccine skepticism.
Many large measles outbreaks in Canada have occurred in insular Mennonite communities in rural Alberta and Ontario, where some are skeptical of vaccines.
Outbreaks have also been reported in Mennonite communities in Mexico and West Texas.
Public Health Ontario has infection numbers for you, broken down by geographic area ("public health units"). Here's what that looks like when I plot them on a graph. Notice that there are five units that are responsible for basically all of the cases, and you will have heard of none of them because they include zero major population centres.
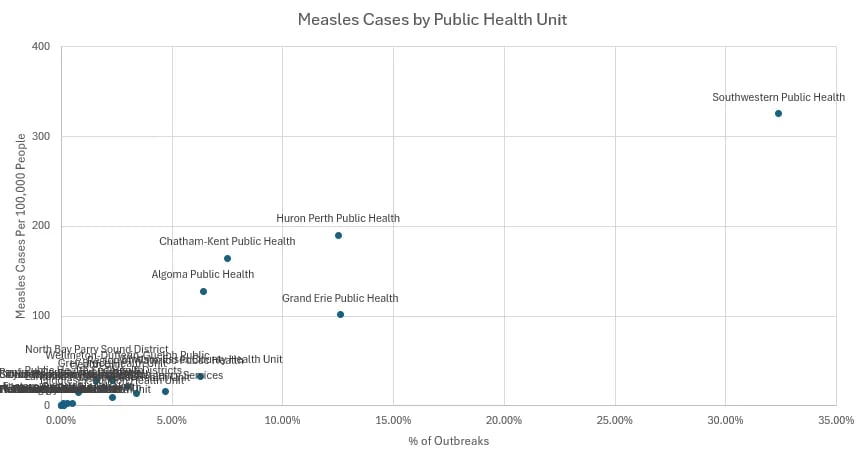
I admit that I do not have the temerity required to separate out Mennonites from like, generic rural dwellers, but something wonky is going on here! The measles outbreaks are all in sparsely populated regions while the big cities (with their big suburbs, presumably where all the anti-vaxxers would be) carry on basically unscathed.
To better visualize this, I am going to combine a bunch of charts together jankily: the geographic distribution of measles (blue), population density (red, adapted from Wikipedia, and, in lime green, the settlements of Amish and Mennonite communities I found online.[3]
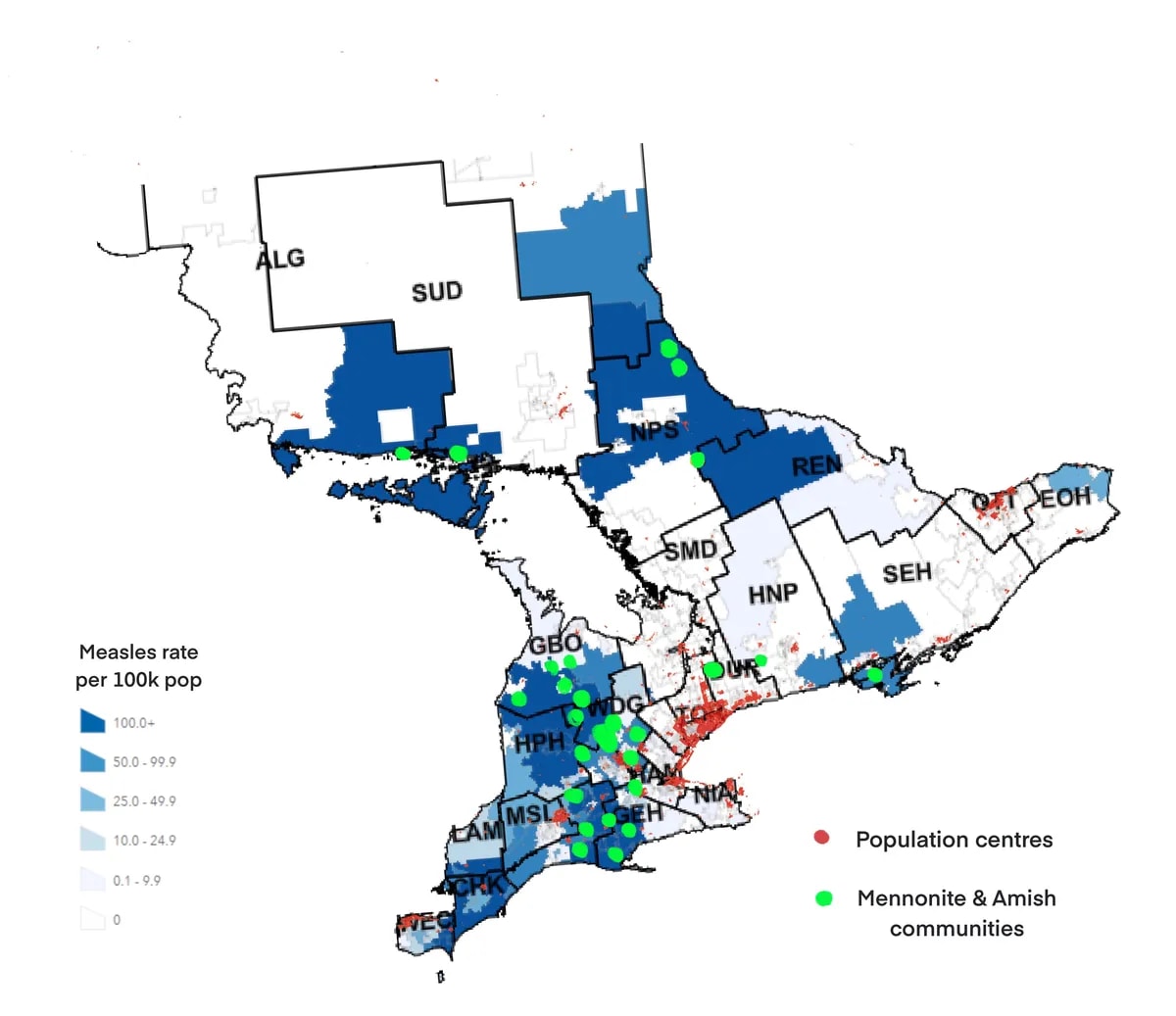
Okay, sorry, you will need to stare at it for a bit. The key takeaway is that the blue areas (which represents measles cases) almost perfectly avoids the most populated areas (red), and are full of green dots (where the Mennonite and Amish settlements are).
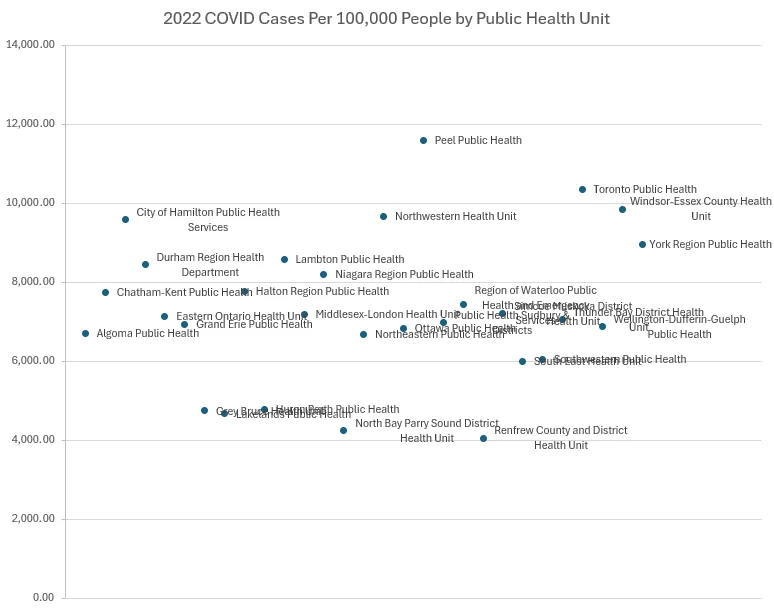
Let's look at this another way. Here's a Public Health Ontario COVID report from April 2022 (i.e. after vaccinations have been available for a while). Pages 8-10 include comparable charts on cases per 100,000 people broken down by Public Health Unit. It's relatively stable between PHUs, and larger in city centres compared to rural settlements. This makes sense, because urban settlements are by definition denser, which means it's easier for viruses to spread.
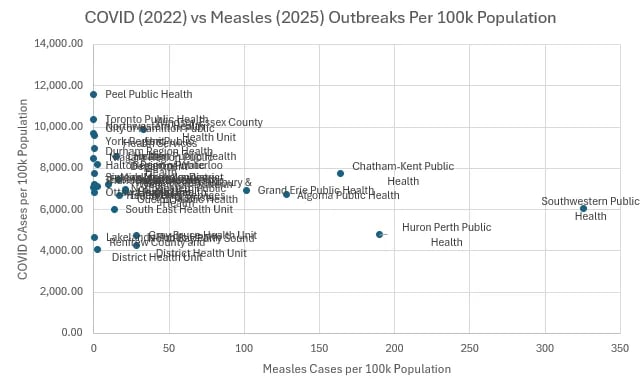
Here are the outbreaks plotted against each other, if you're curious.[4] Notice that the same five public health units no one has heard of are outliers again, which is what you would expect.
Also note the different degrees of variance in cases per 100,000 people in a health unit. COVID cases per 100k ranged from about 4,000 to 11,600 across health units, which is roughly a 3x difference. The Measles cases were actually incredibly discontinuous across units: many units had literally zero cases, some had under 30 cases per 100,000 people, then there's a huge gap, and then there's five regions that had over 100 cases per 100,000 people.
For the statistically inclined, the coefficient of variation (standard deviation divided by mean, expressed as a percentage) was about 25% for COVID and 193% for measles, which is almost eight times higher.[5] (If these numbers mean nothing to you, don't worry about it. The point is just that COVID spread relatively evenly and measles did not.)
Lastly, here is some incidental info from some July 2025 coverage on the outbreak in St. Thomas (a smaller city, in that vertical belt of green dots across central southern Ontario, in the PHU Southwestern Public Health which is the one with the most cases):
Five months later, around 150 to 200 of our [Mennonite] clients have had measles, and most of our Low German–speaking clients have at least had symptoms.
As of October 28, there has been 771 cases of measles in the Southwestern PHU. If 150-200 of them were Low German-speaking mennonites as of July, and most of their clients had symptoms at that time, this indicates that the Mennonites would have made up for a substantial amount of all cases in that PHU.
I rest my case! Which is not to say that it is a perfect one but here is where I put it down because I am not going to put more effort into it. I encourage others to pick it up and put more work into it if they are so inclined.
The general sentiment both in the reddit comments and in most of the news coverage seems to be something like "oh, they're weird religious people, and therefore immune to logic about vaccines", and also something something religious tolerance meaning that we can't criticize their choices at all.[6]
But in reality, Mennonite parents love their children and do not want them to die of measles, and they do not want to contract measles themselves. Having looked into it, it seems to me like the largest barrier for them getting medical care and vaccination is that they are not fluent in English, they speak Low German.
In Ontario, three quarters(!!!!!!) of the 700 Mennonite community clients helped by a Low German-speaking personal support worker have agreed to be vaccinated.
In Alberta (the other large Mennonite population centre, and not coincidentally the other large site of the outbreak), there has been a 25% increase in demand for medical care in Low-German, and service has expanded from five to seven days a week.
And, like, yes, to be clear, there are loads of Mennonites who are actually anti-vaccine. I am not disputing the obvious fact that, in religious communities, many people are against vaccinations. Further, 75% still falls very short of the 92-94% vaccination rate needed for herd immunity. But a 75% vaccination rate is much, much higher than I'd have hoped for?
Here is an example of the miscommunication that can happen when one is not fluent in English:
The following morning, the [Mennonite] mother called me: her child [who recently developed a measles rash] was coughing so violently she was vomiting. I told her to go to the hospital. Later, she called me again, upset. She said that when she got to the ER, they’d told her to go home.
I couldn’t help but think something was off. The hospital doesn’t turn people away, I told her, but she insisted that they had. So I called them directly to figure out what had happened. It turned out there had been a miscommunication. Hospital staff had told her not to come in, using a “stop” hand gesture to communicate, and she had become so flustered that she failed to catch the second part of the message: that she should wait in the car while they prepared a negative-pressure room.
If your measles outbreak comes from this sort of community, the solution isn't to fearmonger about anti-vaxxers. It is to train up and hire health care workers who can speak Low German. And to be clear, I think the PHUs that are affected are doing this, or at least the Ontario ones are, because our public health bodies are generally not disconnected from reality.
And that's what I found most frustrating about the media coverage. It obscures something that's genuinely very hopeful and turns it into another random culture war shitfest. But actually, it turns out that when you remove the actual language and access barriers, people make reasonable healthcare decisions for their families at pretty high rates!
So yes, Canada lost its measles elimination status today. But we can get it back in a year and a bit, if we're serious. And if we're serious about eliminating measles again, we need to focus more on investing in healthcare workers who speak the language of and can build relationships in communities, and less on implying that certain populations are fundamentally unreachable.
This was more true in November, a few comments who made this claim have now been highly upvoted.
There is a trend in the media to avoid naming specific demographics when they are disproportionately involved in bad things. I don't know enough about the soundness of the philosophy behind it to feel like I can comfortably decree "and this is bad", but just for my information diet purposes, it is extremely annoying.
These online sources are sparse for the obvious reason, and are likely somewhat outdated.
There was a health unit merger between 2022 and 2025 so I merged the data in the following ways for cross-comparison:
Claude ran the numbers for me:
Measles outbreak case rate per 100,000 measles = [127.8, 164.3, 0.2, 0, 2.7, 101.4, 28.7, 0.6, 0.3, 190.2, 14.8, 9.9, 2.5, 28.5, 17, 0, 0.3, 0.1, 20.9, 16.4, 2.7, 0.2, 13.6, 325.3, 0, 0.1, 21.1, 33.3, 0.2]
COVID cumulative rate per 100,000 covid = [6707.4, 7747.1, 9581, 8451.9, 7134.7, 6943.7, 4747.7, 4669, 7767.3, 4783.8, 8589.8, 7198.7, 8199.9, 4256.5, 6678, 9671.7, 6840.5, 11594.5, 6979.1, 7440.3, 4056.3, 7218.1, 6000.87, 6056, 7068.2, 10361.8, 6874.5, 9856, 8971]
Measles (n=29): Mean: 38.73 Std Dev: 74.84 CV: 193.2%
COVID (n=29): Mean: 7325.70 Std Dev: 1855.83 CV: 25.3%
Ratio of CVs: 7.6x
We love the Mennonites here the way Americans love the Amish. It's fun, in a way, to dunk on suburban moms, but if you bring up the fact that Mennonites beat their wives and abuse their children it really kills the vibe of the party. I have a huge axe to grind about this, but despite that I do not think it is good for them to die of measles.
{kind=link}